I did a timeline of polio in my last post. Find that here. Please read it first as this post builds on that one.
I want to start with a disclaimer. I do believe that there is an enterovirus called polio that can cause paralysis. I do believe there is a vaccine that creates antibodies to this virus. However, this is obviously an oversimplified view of the story and completely misses large sections of history and ignores factors that decrease the fear of this virus and make one skeptical that the vaccine was actually the sole reason that polio has disappeared here in the US. I don’t want to minimize the horror of paralysis. I have wept reading the case reports, imagining what mothers faced throughout this time with fear of this dread disease that seemed completely arbitrary in its choice of victim, and with no way to combat it or prevent it, watching their healthy children be maimed for life would have been absolutely terrifying and traumatizing. I do not minimize this. But believing that a virus was the sole contributor and that the vaccine was the sole savior is kind of like believing the Christopher Columbus fairy tale we believed in school. The truth is often less pleasant and more complicated.
It’s important to note that poliovirus does not follow the same pattern as any other virus. There are 3 distinguishing characteristics that make it the exact opposite of all other viruses. For one, it was on the rise just as every other virus was decreasing entirely or at least decreasing in its ability to kill and cause permanent harm. If you look at disease morbidity and mortality for all infectious disease, the ability for these infections to cause death had all but disappeared by the 1940s. Poliovirus was on the rise then. Secondly, it was a summer disease. No other virus (that I know of) rises in summer and goes down in winter (unless it’s carried by insects). Thirdly, it affected (almost exclusively) the middle to upper classes and was much lower incidence among the poor.
We now know it was not carried by mosquitoes or any other carrier that was more prevalent in summer. So what made it more prevalent then? Why did it effect the rich more than the poor? Why was it increasing just as all other viruses were decreasing?
In this post, I want to go over some of the factors contributing to the severity and long term effects of paralysis, the different polio vaccines, the issues with each of them, and then finish with present day issues in the East and the problems with pulse polio vaccine programs today.
Contributing Factors:
- Diagnostic criteria
- Introduction of formula to replace breast milk
- Injections–antibiotics and vaccines (provocation polio)
- Tonsillectomies
- Diet
- Environmental Factors (DDT, arsenic, lead, and other pesticides/medications popular in this time)
- Treatment
Diagnosis: I cover the timing of this in my last post, but just to add a little detail, here is a list of conditions (some of which are still prevalent today), that cause the same symptoms as polio, and would most assuredly have been diagnosed as polio before the criteria changed in 1955 and was then further refined to add laboratory testing in 1958. Transverse myelitis, viral or aseptic meningitis, Guillain-Barre syndrome, chronic fatigue syndrome, acute flaccid paralysis, environmental encephalopathy, traumatic neuritis, Reye’s syndrome, enteroviruses such as Coxsackie and ECHO, undiagnosed congenital syphilis, Arsenic and DDT toxicity, provocation of limb paralysis by IM injections of many types, including vaccines, and lead poisoning.
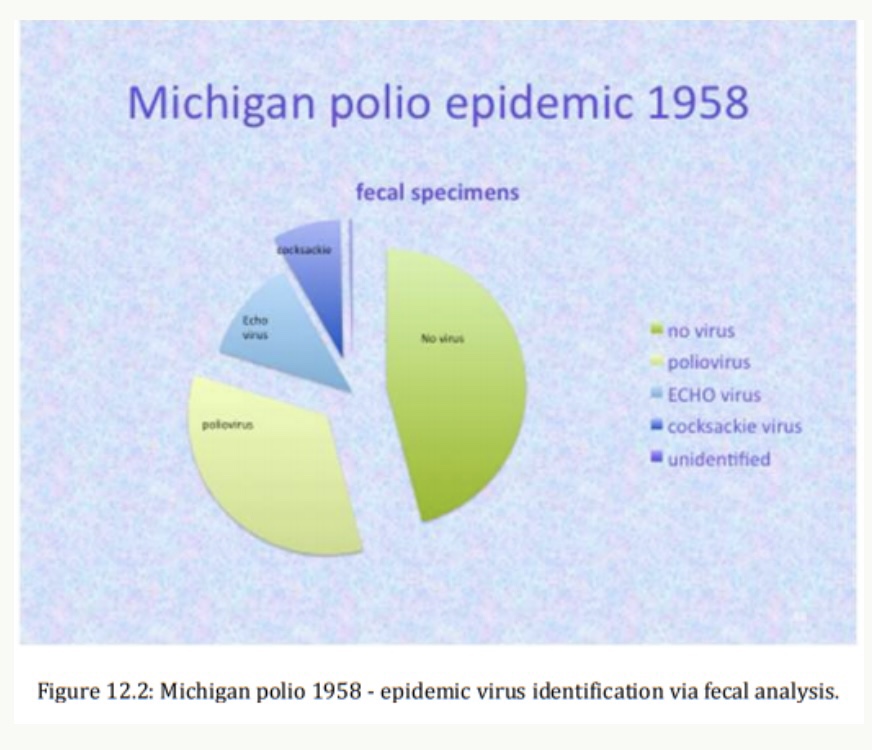
For one glimpse of the diagnostics back then, consider the well-documented Michigan epidemic of 1958. An in-depth analysis of the diagnosed cases revealed that over half of them were not caused by the polio virus at all. [1]
For another glimpse, FDR didn’t have polio after all. [2]
Breastfeeding “Before the late 1800s, all babies were breastfed. If a mother couldn’t breastfeed her baby herself, she would hire a wet nurse. After this time period, primitive powder formulas hit the ymarket. Exclusively breastfed infants were exempt from polio as noted in several epidemics. Those that had other sources of food including cow’s milk and fruit were not exempted, and there’s a reason for that. I think it’s a four fold reason. One was due to lack of maternal protection that’s afforded by breast milk, which is irreplaceable. Second, is due to the toxicity and inferiority of formula, that can never ever under any circumstance, mimic breast milk, which is literally a living organism… Thirdly, DDT given to cows was coming through in the cow’s milk. Cows were treated with DDT, dipped in arsenic, and their milk was toxic. The fourth thing is that formula is basically an immunosuppressant. Now that we know how important bowel flora is, and knowing that 70-80% of our immunity is there. When you look at an infant’s bowel flora that has been fed formula, it is a completely different constitution than a baby who has been fed breast milk.” –Dr Suzanne Humphries
Provocation Polio: Most paralysis in the history of polio occurred in the lower extremities. Occasionally, it affected an arm. The worst kind of polio was bulbar polio, which effected the diaphragm and made people incapable of breathing on their own. Provocation polio is not a conspiracy theory; it is well documented in the medical literature. A large contingent of doctors saw so much injury in this way that they refused to give any injections during polio season because of this. The AMA (after much reluctance) actually got on board with this and advised physicians to delay all “frivolous” injections (including booster vaccines) throughout the summer and fall. [3] The pathophisiology of this is that in the phase when polio virus goes bloodbourne, if there’s any interruption in the tissue or blood vessels, by a needle, for instance, the virus has access to the peripheral nerves and can make its way into the nervous system. The resulting paralysis commonly affects the injected limb, though not always.
Tonsillectomies: Healthy tonsils were removed by surgeons for various financially rewarding but scientifically unsound reasons. 50 to 80 percent of middle-upper class children in the Unites States were needlessly subjected to tonsillectomies in the polio epidemic era. It has been shown in a large group from a 1943 epidemic in Utah that poliomyelitis was more than 2.5 times more prevalent in tonsillectomized children than age-matched non-tonsillectomized children. The incidence of bulbar poliomyelitis (the worst kind) was 16 times higher in tonsillectomized children than in the general child population. 46% of the bulbar polio cases had been preceded by recent tonsillectomy. [4]
Diet: Dr. Van Meer powerfully connected the consumption of white sugar and poliomyelitis epidemics. He makes a convincing argument. [5] Dr Sandler organized an experiment that kind of blows my mind. In 1948, North Carolina had the 2nd highest rate of poliomyelitis in the country, and after his broadcasting campaign, warning the public of sugar consumption and its link to polio, he was effective in getting people to actually change their eating habits, and by 1949, North Carolina saw a 90% drop in poliomyelitis cases. They went from 66.3 per 100,000 in 1948 to 6.3 in 1949. [6,7]
I go over DDT toxicity and its comparison to polio in my previous post. Suffice to say that lead toxicity has the same list of symptoms and was often confused for poliomyelitis.
I want to go over arsenic because you might not realize it was actually used in medicine at this time. Arsenic was actually very prevalent, right around the time that polio was at its height. On top of being heavily sprayed on crops, it was used in household and medical products. Arsenic was used to treat lung problems; doctors would add it to tobacco to be smoked (yes, doctors heavily promoted smoking and tobacco during this time as well). Arsenic was used by dentists to kill nerves in decayed teeth. Arsenic was approved in medicines by the AMA. One of these medications was called tryparsamide, manufactured by Merck, licensed in 1939, used in the treatment of syphilis, often with 100 injections in a single patient. Yes, I did a double take as well. That’s not a typo. Here’s a very matter-of-fact case report for one example: “Another patient who had previously received thirty-four injections of arsphenamine (another medicine containing arsenic), twenty-three injections of bismuth, and seventy-six mercury rubs had a paretic type of serologic relapse after 104 injections of tryparsamide.” [8] No one must have told these doctors that the dose makes the poison.
Dr Scobey proved that arsenic was a cause of poliomyelitis (inflammation of the gray matter of the spinal cord). This article was later used to testify against arsenic to the house of representatives. [9]
Treatment: “We’d take the children to the operating room in those days, straighten them out under anesthetic, and put them in plaster casts. When they woke up, they screamed. The next day they still cried from the pain. That was the accepted and universal treatment virtually all over the world.” [10] Affected limbs were routinely immobilized in casts for 3-6 months and often as long as two years.
We know now that immobilization leads to muscle weakness and can cause permanent damage if done for long enough, even in healthy limbs.
Sister Kenny, a pioneer of what is now known as physical therapy worked tirelessly against the belief system that said splinting was the best treatment. It took her 30 years to get the orthodox medical community to accept that they had been incorrectly treating polio and were thus responsible for much of the residual paralysis, deformities, and lingering stiffness. Even after her success was unquestioned, she was only allowed to treat the failures of other physicians. One can imagine how much suffering would have been prevented if doctors would have adapted her methods instead of fighting her so militantly. The children probably looked a little like this photo taken in Nigeria in 2005, demonstrating how hard it is for old habits to die, regardless of poor outcomes.
The treatments also included things like tendon cutting and transplantation, and other such “savage operations“, prolonged splinting, surgical straightening, and painful but ineffective electrical treatments. [11] “Orthopedists believed in the “extreme fragility” of poliomyelitis muscle. Many victims of this disease were cast in plaster for 6 months or so, and their deformities were operated on in due course. Not even massage–much less vigorous exercise of the affected muscle was countenanced.“ [12]
Besides Sister Kenny, other doctors were also treating polio with much more success than the mainstream efforts to immobilize and torture. Dr Klenner cured 60 out of 60 patients of polio (including bulbar polio) with high dose, intravenous vitamin c. [13] Two other doctors used vitamin c successfully. [14, 15] It’s ironic that those who were reporting success in their treatment went ignored for 30 years and ignored completely by the history books, as is the case for the doctors using vitamin c and those talking about diet. Maybe these treatments were so simple and easy that they appeared too good to be true? One would assume doctors of the time would at least try something that their colleagues were saying was successful, especially since none of these treatments came with any risks. But sometimes, humanity becomes entrenched in the collective approach despite the fact that it yields inferior or no results. Or maybe it’s just the arrogance of not wanting to admit you’re wrong. That’s definitely a powerful drive.
Now, on to the vaccines…
1955 was when the first polio vaccine was introduced. It was Dr Salk’s inactivated polio vaccine (“inactivated” is quite a stretch). The Salk vaccine was approved just after being developed and fast-tracked into licensure by the US Department of Health, Education, and Welfare. This approval process took a record-breaking two hours. [16]
This approval process and the way it was put on the market was fascinating and well documented. For example, “Jonas Salk had a paper in which he argued that all the virus was inactivated, and that there was no live virus left. But, the sixth lot was not listed. And so I said that something was wrong. He cut out data in order not to show what happened to some lots…Well, NFIP did form an advisory committee. And they reformed it five or six times. Each time somebody didn’t agree, they dropped them and got somebody who might agree. By the time they were done forming the committee, everybody on it was distinguished, but very agreeable.” [17]
As a result of ignoring the warnings by highly qualified scientists who repeatedly and publicly explained why and how the inactivation process was flawed from the beginning, the vaccine infected, paralyzed, and killed children and their household contacts. This became known as the “Cutter Incident“.
Between April 17 and June 30, 1955, 260 poliomyelitis cases were documented after inoculation of about 400,000 persons with the Cutter vaccine. 94 cases were among vaccinees, 126 among family contacts, and 40 among community contacts. An estimate of the case-infection ratio is in the range of 1 case per 100 to 600 injected infections. [18]
“In the end, at least 220,000 people were infected with live polio virus contained in Cutter’s vaccine; 70,000 developed muscle weakness, 164 were severely paralyzed, 10 were killed. Seventy five percent of Cutter’s victims were paralyzed for the rest of their lives.” It is admitted by the most staunch vaccine advocates that, “…the disease caused by Cutter’s vaccine was worse than the disease caused by the natural polio virus.” [19] This is a conservative estimate of the damage. Scientists at the time admitted this vaccine may have caused much more damage than was being reported.
Most mainstream stories of polio ignore the Cutter Incident altogether, but if they do cover it, they blame Cutter laboratories. They ignore the fact that all manufacturers had documented difficulty killing the virus in their vaccines, before and after the disaster. [20] And Cutter was not the only lab producing an “inactivated” vaccine that was injected into children and caused paralysis. [21]
The inactivated polio vaccine is still inactivated by the use of formaldehyde. The balance must be difficult to achieve. You must kill enough of the virus that it doesn’t cause paralysis, but leave enough so that an antibody response is obtained, and the more formaldehyde you use, the more toxic the vaccine becomes. Formaldehyde is used in embalming, is listed as a carcinogen, and is toxic to life (why it is useful in “killing” viruses). Children in the US receive 4 doses of inactivated polio vaccine by the time they are 5 (3 of those by 15 months).
SV40 Simian virus number 40, is a monkey virus that has been found in several types of cancers, including lung mesotheliomas, several types of brain tumors, and bone, breast, colon, and kidney tumors. [22] Vaccines manufactured using monkey kidneys up into the 1980s have been definitively noted [23] to contain a carcinogenic monkey virus that can result in cancer in a portion of the millions who were given them. [24]
“How a virus dubbed “the perfect war machine” by Dr Carbone because it affects at least four major cellular mechanisms that either promote cancer or interfere with cancer-fighting defensese, could be impacting countries that continue using oral polio vaccines by the ton today, is anyone’s guess. How much of the abrupt rise in human cancer rates since the introduction of monkey products into the human population is due to SV40 will also remain uncertain due to lack of precise research.” –Dissolving Illusions
Monkeys are still used in polio vaccine production today. According to Stanley Kops’ allegations, SV40 was and still is a potential risk in both the OPV and the inactivated polio vaccines. The only vaccine that doesn’t use monkey kidney cells, uses aborted fetal tissue instead. [25, 26] (page 15 and page 11)
Interesting side note, both of the rotavirus vaccines today are contaminated with two different pig viruses called “porcine circovirus (PCV) 1 and 2. …not known to cause disease in humans”. [27] Very reassuring, since there’s no way to know if it causes disease or not until after it’s too late, unless they were to study this type of thing. Anyone want to take a stab at whether or not they’re doing studies, or maybe recalling these vaccines until they’re certain?
Fast forward to present day. No wild polio virus in the Western Hemisphere, barely any in the entire world, in fact. In 2017, there were only two cases of wild polio virus causing paralysis. Most years, its well under 10. But is that good enough? Not even close. It must be stomped out at all cost. And I do mean at all cost. So the war marches on. And there are casualties. All worth it, I’m sure. This is war, after all. A few casualties are worth it in the name of eradicating a disease.
What about paralysis? How is that going? Now that we have new diagnoses for things that would have fallen under the polio criteria, does anyone know the numbers? What about children on ventilators? Some people celebrate the fact that we no longer have people in iron lungs…but the threat of returning people to iron lungs is almost as ludicrous as threatening the “return” of polio.
In India, as the WHO (world health organization) tracks polio during the vaccination campaigns, reports of paralytic cases associated with wild-type poliovirus have declined, and AFP (acute flaccid paralysis) has increased annually, reaching 60,000 new cases in 2011.
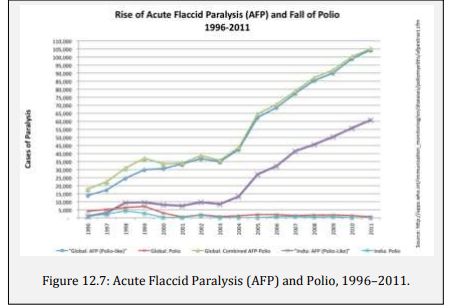
It just so happens that DDT is still heavily used in India. And the cause of AFP is, of course, a huge mystery to everyone.
The OPV (oral polio vaccine) was discontinued here in the US in 2000 because of the contamination of vaccine strain polio in our water sources along with multiple complaints of paralysis after the vaccine, but it continues to be used aggressively around the world, some reports say an Indian child is vaccinated with live vaccine 15 times by the time they are 5. [28]
24 of the last 26 outbreaks of polio in the world have been caused by the oral polio vaccine over the last 6 years. [29] This is undisputed fact. How much paralysis and damage and death is that? After 6 years (much, much longer, if we’re being honest) of causing more suffering than you are preventing, isn’t it time to just back off and leave nature alone? But no. The battle continues. Any price is worth it when you’re not the one paying it.
It has been reported in the Lancet that the incidence of AFP, especially non-polio AFP, increased drastically in India after an experimental, high-potency polio vaccine was introduced. [30] Worse still is that children identified with non-polio AFP are at more than twice the risk of dying than those with wild polio infection. [31] Shouldn’t eliminating paralysis be more important than simply replacing wild virus with vaccine virus regardless of the outcome? It seems that paralysis itself is nothing when compared to the horror contained in the tunnel vision of disease eradication.
Is it possible to eradicate something with a vaccine that causes the disease it’s trying to get rid of?
What about paralysis here in the US?
Dr Douglas Kerr from John Hopkins states, “Infants as young as five months old can get transverse myelitis, and some are left permanently paralyzed and dependent upon a ventilator to breathe…my colleagues at the Johns Hopkins Hospital and I hear about or treat hundreds of new cases every year.” [32] Does the public have any idea that there are hundreds of cases of something that is now called transverse myelitis that would have historically been called polio and is now leaving children permanently dependent on a modern version of the iron lung?
Approximately 33,000 people are afflicted by transverse myelitis in the Unites States, with 1,400 new cases per year. And this is just one condition that would have been called polio back in the day.
What causes transverse myelitis? No one seems to have identified a sole cause, but the National Institute of Health lists vaccines as one of the causes, [33] and it’s listed in the adverse events or postmarketing surveillance sections of almost every vaccine package insert. It’s listed on page 5 of the varicella insert, for example. [34] I bet people would be shocked to find that an unlucky few are making the choice between their child being permanently paralyzed and a few days of chicken pox.
This article from last year was quite eerie to read after all the case reports I’ve been reading lately. Quotes like the following had a shiver going up my spine at the connections being so completely missed. “Government health officials are urging U.S. doctors to be on the lookout for a mysterious condition that has begun to re-emerge in late summer and early fall, targeting healthy young children and leaving them paralyzed. There have been about 570 cases to date.
There is no known way to prevent or treat it, and doctors are still unable to predict which children will develop paralysis. For those who do, the paralysis and weakness can last for months and it’s unclear how many will fully recover.
“We want clinicians and parents to be ready for a possible significant outbreak this year,” Anne Schuchat, principal deputy director of the CDC, said on a conference call with reporters. “One of the reasons we are reporting these results right now in July is because it’s every August that we start to see the uptick.”
Identifying potential patients early in the course of the disease is critical since the condition can quickly spiral from limb weakness to full-blown respiratory failure that requires intensive medical care, according to the CDC. Children who get the condition tend to be about 5 years old.”
What happens in August to five-year-olds? Hmmm. But I’m sure before-school-shots have absolutely nothing to do with this. It’s all a coincidence.
- https://jamanetwork.com/journals/jama/article-abstract/327642
- https://www.ehdp.com/out/jmb_2003_v11_p232-240.pdf
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61251-4/fulltext
- https://www.sciencedirect.com/science/article/abs/pii/S0022347645802081
- https://pdfs.semanticscholar.org/c46b/1d6f49671d77c27d005280609459b495cbb8.pdf
- https://www.seleneriverpress.com/images/pdfs/864_SANDLER_NEWSPAPER_REPORTS.pdf
- https://books.google.com/books?id=31QtmHLg77IC&pg=PA116&lpg=PA116&dq=dr+sandler+north+carolina+white+sugar&source=bl&ots=pqG95xVmvb&sig=ACfU3U2IGsSY9qJeOhBn-0xd-sgfK3f1DA&hl=en&sa=X&ved=2ahUKEwi2hp64woboAhXvknIEHRVFA2QQ6AEwAnoECAoQAQ#v=onepage&q=dr%20sandler%20north%20carolina%20white%20sugar&f=false
- https://sti.bmj.com/content/sextrans/10/2/99.full.pdf
- http://whale.to/a/scobey2.html
- J. R. Paul, A History of Poliomyelitis, Yale University Press, New Haven, Connecticut, 1971, pp. 335-339.
- Victor Cohn, Sister Kenny: The Woman Who Challenged the Doctors, University of Minnesota Press, 1975, p. 5.
- S. Mead, “A Century of the Abuse of Rest,” Journal of the American Medical Association, vol. 182, October 1962, pp. 344-345.
- https://www.seanet.com/~alexs/ascorbate/194x/klenner-fr-southern_med_surg-1949-v111-n7-p209.htm
- https://www.seanet.com/~alexs/ascorbate/195x/greer-e-medical_times-1955-v83-n11-p1160.htm
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2133810/
- Richard Carter, Breakthrough: The Saga of Jonas Salk, Trident Press, New York, 1955, p. 282.
- https://journals.sagepub.com/doi/abs/10.1191/1740774504cn011xx
- https://academic.oup.com/aje/article-abstract/142/2/109/116270?redirectedFrom=fulltext
- Paul Offit, MD, The Cutter Incident, Yale University Press, 2005, p. 89.
- https://jamanetwork.com/journals/jama/article-abstract/301686
- A. Langmuir and N. Nathanson, “The Wyeth Problem”, September 6, 1955.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3241931/
- https://cancerres.aacrjournals.org/content/65/22/10273
- https://cancerres.aacrjournals.org/content/59/24/6103
- https://www.gsksource.com/pharma/content/dam/GlaxoSmithKline/US/en/Prescribing_Information/Pediarix/pdf/PEDIARIX.PDF
- https://www.fda.gov/media/91640/download
- https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/b/excipient-table-2.pdf
- https://www.researchgate.net/publication/6686398_New_Strategies_for_the_Elimination_of_Polio_from_India
- https://web.archive.org/web/20201121204818/https://www.who.int/csr/don/archive/disease/poliomyelitis/en/
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(07)60531-5/fulltext
- https://www.ncbi.nlm.nih.gov/pubmed/17642508
- https://www.goodreads.com/book/show/1635281.The_Autoimmune_Epidemic
- https://web.archive.org/web/20170320181509/https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Transverse-Myelitis-Fact-Sheet
- https://www.merck.com/product/usa/pi_circulars/v/varivax/varivax_pi.pdf
